 Mast cells are found throughout the body, particularly at the interfaces with the outside world (such as the GI tract, the respiratory tract and the bladder) and are meant to be sentinels on the lookout for invaders that can potentially cause harm to the organism. As such, they are armed with an impressive array of weapons in the form of chemical substances that can neutralize and kill foreign organisms or toxic compounds. The triggering and release of mast cell activity must be exquisitely balanced such that protection does not fail yet no harm comes to the body itself. It has been determined in recent years that mast cells can release their dizzying variety of bioactive chemicals with little or no apparent provocation and thus cause sometimes severe symptoms in virtually any site in the body.
Mast cells are found throughout the body, particularly at the interfaces with the outside world (such as the GI tract, the respiratory tract and the bladder) and are meant to be sentinels on the lookout for invaders that can potentially cause harm to the organism. As such, they are armed with an impressive array of weapons in the form of chemical substances that can neutralize and kill foreign organisms or toxic compounds. The triggering and release of mast cell activity must be exquisitely balanced such that protection does not fail yet no harm comes to the body itself. It has been determined in recent years that mast cells can release their dizzying variety of bioactive chemicals with little or no apparent provocation and thus cause sometimes severe symptoms in virtually any site in the body.
If you have been diagnosed with MCAS or suspect you may be suffering from the effects of overactive mast cell mediator release this article will attempt to clarify some of the underlying pathologies that manifest in the form of MCAS.
Let’s start with perhaps the easiest one to understand – histamine sensitivity. Histamine causes many classic reactions in the body such as dilation of blood vessels and release of fluid (“runny nose”) as well as itching and hives. If you ingest or inhale something to which you are allergic, you expect your mast cells to release histamine and you know what allergy symptoms to expect. But if your mast cells are releasing histamine at inopportune moments, you may be itching and swelling for no apparent reason. It may become very frustrating to try to find out and avoid whatever is causing these symptoms and the only recourse may be taking histamine blockers (“antihistamines”).
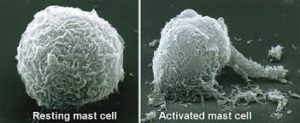
Similarly, MCAS can result in excessive release of many other mast cell mediators (at last count around 200 separate mediators have been identified in the mast cell!). Mast cells contain secretory granules that release chemical mediators when they are activated. These mediators are divided into three categories: preformed mediators (histamine, serotonin, and others), newly-synthesized lipid mediators (prostaglandins and others), and cytokines and chemokines (interleukins, TNF-alpha, and others). Each of these mediators has specific targets or receptors. Histamine tends to get the most time in the spotlight but it is important to know that there are other mediators that are released in various parts of your body and this may account for a variety of symptoms you may experience. Each mediator has direct effects, indirect effects, and remote effects so when you put all of these together it is easy to see why exact diagnosis can be so elusive at times.
The diagnosis of MCAS depends upon the detection of the products of mast cell activity in blood and urine samples. Some of these (such as tryptase) are unique to mast cells and others are less specific but no less clinically significant. Elevated serum norepinephrine levels may be due to mast cell overactivity. Chromogranin A, heparin and Factor VIII may also be indicators. In 24 hour urine collections N-methylhistamine, PGD2 and 11-beta-PGF2alpha can also be detectable markers. These and many other substances can be vital clues to MCAS.
Treatment is generally aimed at preventing the mediators from docking with their targets, eliminating the introduction of known mast cell triggering substances, stabilizing the mast cell membrane itself and neutralizing or counteracting the effects produced by the mediators in their target organs.
The recent release of NEVER BET AGAINST OCCAM BY Dr Lawrence Afrin, an acknowledged expert in the field of MCAS, has contributed greatly to the expansion of our recognition of this disease complex. I highly recommend and refer to this book frequently in my discussions with patients and colleagues.
The search is on and in many ways is just beginning to effectively diagnose and treat this sometimes bewildering syndrome. We are certainly making progress but have many paths yet to explore.